Vestibular Neuritis/Labyrinthitis
Background:
Signs and Symptoms:
Vestibular Neuritis:
Labyrinthitis:
Diagnosis:
Treatment:
Vestibular Neuritis:
Special Tests:
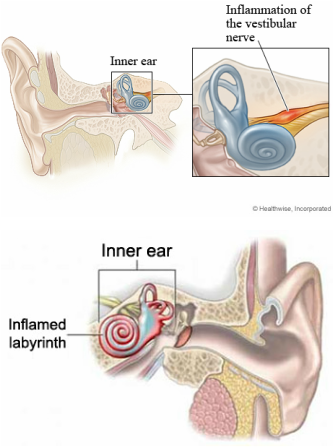
- These terms are often used interchangeably in the the literature, although they are similar conditions, they have minor differences. Vestibular Neuritis is also referred to as Vestibular Neuronitis, it is an infection of the vestibular nerve (CN VII). This condition manifests as a viral infection and commonly follows an episode of the flu (Post, 2010). Labyrinthitis is also an infection, but it affects the labyrinthine organs of the inner ear. Viruses such as: influenza A, Rubella, Mumps, Cytomegalovirus, Enterovirus, and various bacterial infections may cause this inner ear problem (Simonsen, 1996). Both of these conditions are peripheral in nature and may be referred to collectively as, Vestibulopathy (Simonse, 1996).
Signs and Symptoms:
Vestibular Neuritis:
- Persistent vertigo (Post, 2010)
- No hearing loss (Post, 2010)
- Rapid onset, severe rotary vertigo (Lee, 2012)
- Nausea and vomiting (Lee, 2012)
- Severe imbalance (Lee, 2012)
- Symptoms can last from days to months (Lee, 2012)
Labyrinthitis:
- Persistent vertigo (Post, 2010)
- Hearing loss (Lee, 2012)
- Sudden attacks of vertigo (Simonsen, 1996)
- Spontaneous nystagmus (Lee, 2012)
- Bacterial causes may result in ear discharge (Lee, 2012)
Diagnosis:
- With vestibular neuritis, the involved ear will have a decrease caloric response (Lee, 2012).
- With labyrinthitis, many patients experience an upper respiratory tract infections before the onset of vertigo. Serologic evidence of acute viral infections, or activation of latent viruses may also be present (Simonsen, 1996).
- With labyrinthitis, an early ENT assessment should be done to rule out underlying Cholesteatoma or chronic Suppurative Otitis Media, which requires surgical management (Lee, 2012).
- With suspension of either condition, the patient should be checked for nystagmus (Lee, 2012). (See Special Test Tab)
- The nystagmus will be horizontal or torsional and can be suppressed with visual fixation (Lee, 2012).
- For both of these conditions, a diagnosis should be based on the patients history, hearing loss, and duration of symptoms (Post, 2010).
Treatment:
Vestibular Neuritis:
- Vestibular sedatives can be used early on, for short periods of time, but should be tapered down over several weeks (Post, 2010).
- For long-term use, a vestibular sedative is not recommended, as it prevents central compensation and slows recovery (Lee, 2012).
- Vestibular rehabilitation speeds recovery and improves symptoms in up to 80% of patients (Lee, 2012). (See Treatment Tab)
- Sedatives and antibiotics should be given to relieve acute symptoms and treat the underlying infection (Lee, 2012).
- A short course of vestibular rehabilitation is often prescribed with the same goals indicated for vestibular neuritis (Beyea, 2012). (See Treatment Tab)
- Vestibular exercises are used to enhance and strengthen the vestibule-ocular reflex, static and dynamic stability, and activities to improve tolerance to head and body movements (Kaylie, 2012).
- Optimal management includes a combination of medication and vestibular rehabilitation (Alghadir, 2013).
Special Tests:
- The Head Shaking Test for 20 seconds should be used to induce nystagmus (Post, 2010). (See Special Test Tab)
- The presence of nystagmus indicates a peripheral cause in the direction of the nystagmus (Post, 2010)
- Romberg Test and observation of gait should also be assessed. Swaying towards one side during the Romberg indicates vestibular dysfunction on the ipsilateral side (Post, 2010). (See Special Test Tab)
